Dr Arnaud STANURSKI Endodontics and Implantology specialist 125 Avenue du Bac
FR-94210 - LA VARENNE SAINT HILAIRE
FRANCE  Clinical case commented by Pr. Jean-Marie Vulcain Case introduction:- Upper left second molar, tender on biting and to percussion tests
- Failing coronal restoration with evidence of a loss of coronal seal
- Previous obturation inadequate
The pre-operative radiograph reveals:
- Under-obturated canals in the apical third
- Lack of coronal seal
- A glass fiber post present in the palatal canal
- After discussion with the patient, it was agreed that endodontic re-treatment is indicated 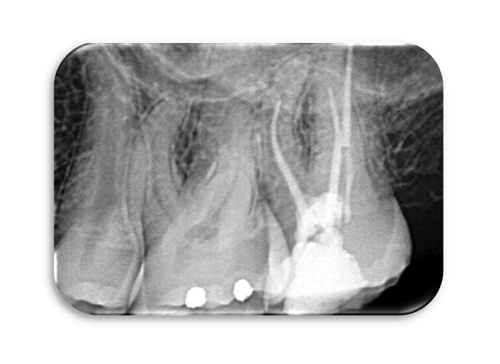 Re-treatment under operating microscope - Setting up of the operative field
- Removal of the coronal obturation
-Access cavity refining.
- Preparation with ultrasonics to identify and expose the canal orifices.
- Placement of a well-sealed provisional coronal restoration  - Removal of coronal filling material with ultrasonics
- Removal of the obturation in the mesial canal with Neoniti A1 no. 20/.06 file used at 650 rpm / 1 N.cm
- Patency of canals with a C+ size 10 file from Dentsply then with Neoniti GPS no. 15/.03
- Measurement of the Working Length (WL)
- Meticulous preparation of the canal walls using brushing motions and thorough irrigation.
Always using Neoniti A1 no. 20/.06 file and then Neoniti A1 n°25/.06
- Please notice the double curvature of the disto-buccal root and the mesio-buccal root curvature
- Drying of the canals
- Obturation by warm vertical condensation or by thermo-compaction 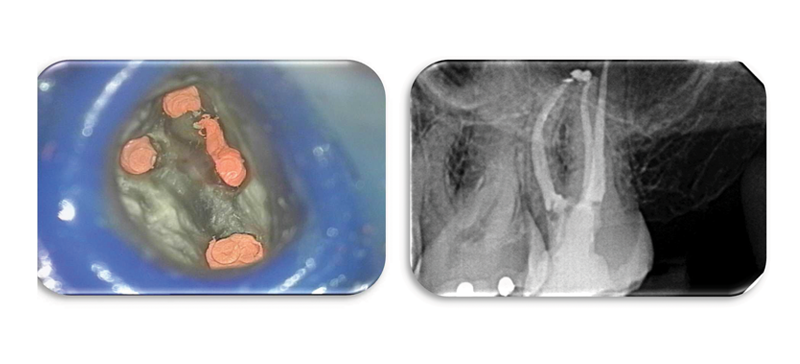 - Finally, placement of a coronal seal over the gutta percha followed by a core material and subsequent, definitive restoration of the tooth Comments This is a complex clinical case. The canal obturations are limited in their length, volume and density. There is also fiber post in the palatal canal. Moreover, the coronal restoration is defective, and access to the upper second molar is often a challenge.
The removal of the old obturation material was easily achieved and the use of the operating microscope facilitated the identification of the original three canals and the additional MB2 missed in the original procedure.
Refining of the opening of the access cavity and the relocation of the MB and MP orifices made access to the apical third of the MB canals easier and ensured apical patency was achieved. This stage is crucial especially when visual access is limited.
The images taken under the microscope during the procedure clearly demonstrate the identification of the canal orifices, the complete removal of the old filling material, the efficient and conservative canal shaping, and finally the new obturation with warm gutta percha. This result is possible thanks to the careful use of hand instruments, ultrasonic instruments, the action of Neoniti A1 no. 20/.06, and use of thermo-injection system for gutta percha. Endodontic retreatment to retrieve a broken instrument. Pre-operative radiographs show:
- The presence of widening of the periodontal ligament space around the mesial root suggesting persistent peri-radicular infection.
- The presence of two fragments of separated endodontic file in one of the mesio-lingual canal.
- The potential for a ledge having been created at the type of the fractured file.
- Inadequate coronal flare to the canal making access to the apical third difficult and likely contributing to the fracture of the file. 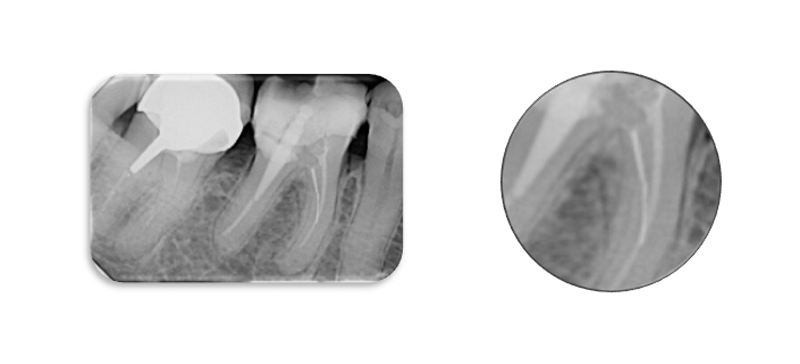 Comments The two instrument fragments were removed using ultrasonic files. A ledge was detected as anticipated.  This ledge was negotiated by pre-bending instruments, initially handing files such as a size 10 but then also we have the benefit of being able to pre-curve Neoniti files and to eliminate ledges by preferentially brushing the wall of the canal.
Modern manufacturing processes mean that files such as Neoniti A1 have significantly improved shaping ability. Neoniti A1 files are manufactured using a unique electric machining process followed by proprietary heat treatment resulting in a very flexible file discharge with a hardened, abrasive surface. | Dr Jérémie BOISSEAU Specialist in Endodontics 35 B Chemin des Graviers Blancs
FR-25000 – BESANÇON
FRANCE  Clinical case commented by Pr. Jean-Marie Vulcain Case introduction: The patient reported severe pain and swelling from the upper right second molar (17). There was tenderness on biting and swelling buccally. The tooth was restored with a metal ceramic crown.  Radiographically it was obvious that the tooth had been previously root treated and that there was:
- Evidence of persistent periapical pathology and bone loss associated with the buccal roots
- The previous root appeared filling to be well condensed and of adequate length
- An inlay-core was present as well as a post within the palatal root
- There is a suggestion of some space beneath the inlay-core, possibly indicating the unsealing of the cement. Planned retreatment - Removal of the crown and the inlay-core
- Inspection and assessment of the remaining tooth tissue under the crown 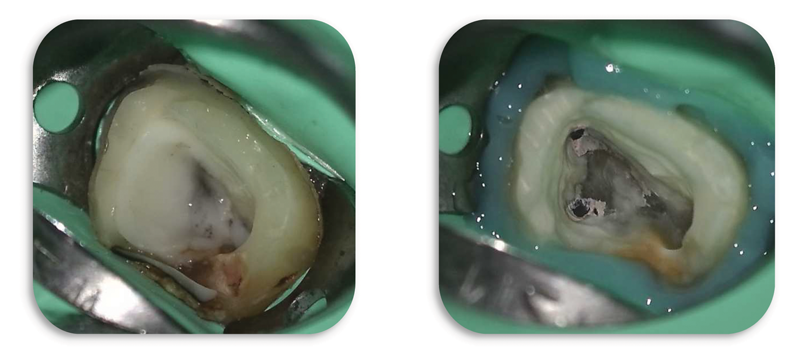 Removal of the remnants of the Glass Ionomer Cement, caries removal and creation of a cervical seal. Initial inspection under the endodontic microscope revealed the presence of a previously untreated MB2 canal. It also became clear that the previous obturation had been completed using a carrier based device, possibly Thermafil.  Removal of the carrier based obturation (Thermafil) -Access cavity preparation
- Ultrasonic preparation uncovering the root canal entries including the MV2 canal
- Use of Neoniti C1 25/.12 and then irrigation
- Root canal patency with Neoniti GPS file, with thorough irrigation at each stage
- Working Length (WL) determination
- Careful shaping of the canal, using the wall brushing technique ensuring that all areas of the canal are prepared including the ones not treated yet with Neoniti A1 no. 20/.06 and A1 no. 25/.06. 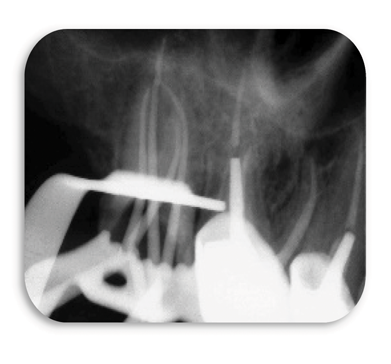 Intraoperative radiography with master cones in place and clinical view of the tooth after root canal preparation.  It should be noted the presence of the 4 channels (including the MV2) with their curvature - Drying of the root canals
- Obturation by warm vertical condensation of the apical third and coronal backfill with injected heated gutta percha. Only the apical half of the palatal canal was obturated, leaving space for the placement of a post
- Each stage of the procedure was performed with the assistance of a surgical microscope. 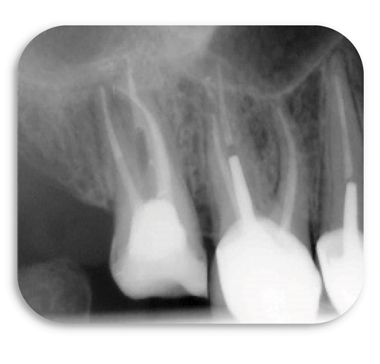 Postoperative radiography of provisional coronal filling  Clinical view after obturation - The tooth was provisionally restored ensuring a good coronal seal and the definitive restoration of the tooth was scheduled a few days after the endodontic procedure. Re-treatment of the upper left first molar #26. 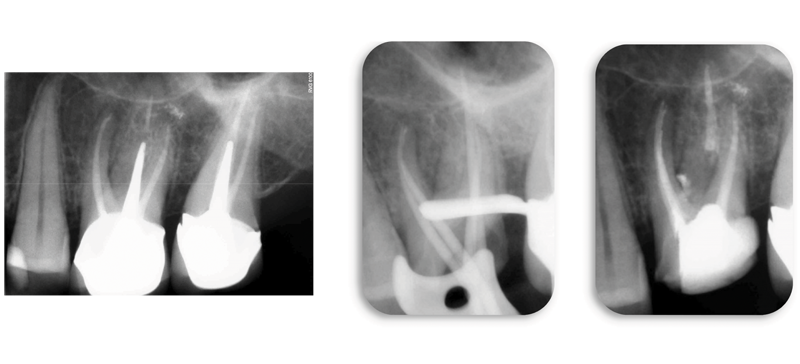 The presence of persistent periapical bone loss associated with the mesial root of the upper right first molar indicates the need for non-surgical re-treatment of this tooth. The procedure was performed in the same way as Case 1 and the postoperative radiograph shows the presence of a large lateral canal in the coronal third of the mesial root. The treatment of the additional MB2 channel is also evident. Summary of these cases: These two cases highlight that endodontic success can only be expected if the treatment is performed with careful adherence to the essential principles of shaping, cleaning, obturation and the provision of a coronal seal. In these cases endodontic retreatment was required. The successful revision of a root treatment, requires a very careful removal of the previous root filling, achieving apical patency and the thorough debridement of the canal space, including preparation of the canal walls using the technique of wall brushing motions to facilitate the thorough irrigation of the root channel system.
The smart use of only 4 Neoniti instruments (C1 no. 25/.12, GPS no. 15/.03, A1 no. 20/.06 and A1 no. 25/.06) resulted in:
- The retreatment of the canals respecting the fundamental principles of endodontics. - Dense three-dimensional obturation by warm vertical condensation. - The subsequent placement of well-sealed and functional coronal restorations.
Ultimately, two teeth that would otherwise have been extracted, were preserved and will serve the patient well for many years. | Dr Jean-Louis MERCIER General Practitioner Zac de Beauvais – 2 Rue des Mérisiers
FR-35500 VITRE
FRANCE  Clinical case commented by Pr. Jean-Marie Vulcain Case introduction: The upper left first molar #26 has a large coronal alloy restoration. This tooth has been the source of intense episodic pain. A diagnosis of irreversible pulpitis was made and the tooth was scheduled for Initial Endodontic Treatment. The preoperative radiograph shows:
- Extensive coronal restorations in all of the teeth in this quadrant
- The presence of a post crown in an un-root filled premolar tooth
- Generalized horizontal bone loss
- In the tooth #26 we can see a large coronal restoration
- Significant pulpal and canal sclerosis This tooth represents a challenging endodontic treatment. 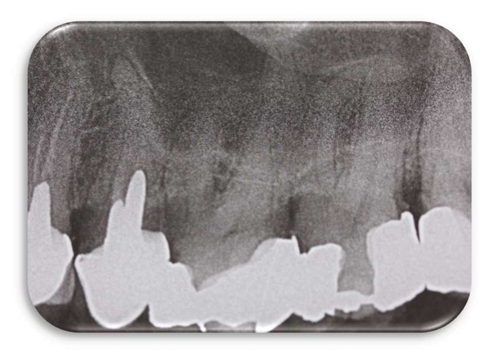 Initial endodontic treatment - Local anesthesia
- Isolation with rubber dam
- Accessing the pulp chamber
- Location of the canal orifices with a DG 16 probe under magnification and with thorough irrigation
- Opening of the root canal entrances with Neoniti C1 no. 25/.12 and then irrigation
- Initial glidepath with stainless steel #10 K-files
- Completing glidepath with Neoniti GPS no. 15/.03, and irrigation
- Measuring the Working Length (WL) using an apex locator
- Shaping the root canals with Neoniti A1 no. 20/.06, then A1 no. 25/.06, and irrigation
- Drying of the root canals
- Obturation by pre-calibrated master cones
- Final radiographic examination 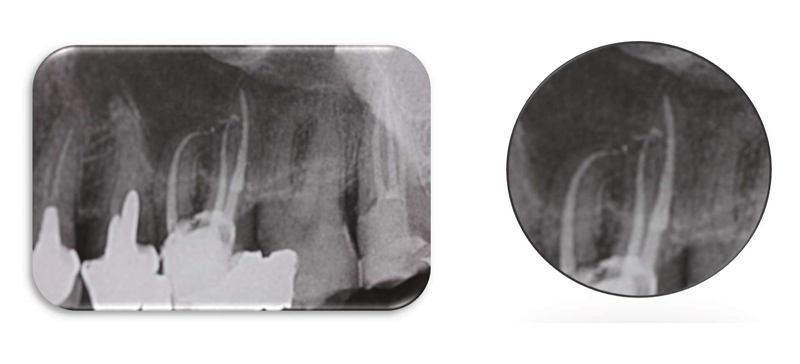 Comments The use of the Neoniti system enabled the treatment to be completed efficiently in a single visit. The shaping respects the natural shapes and curvatures. Careful measurement and control of the working length resulted in a well cleaned and obturated canal system with a very satisfying final result.
The Neoniti shaping procedure, allows complex shapes to be prepared routinely and hassle-free. Open the canals with Neoniti C1 no. 25/.12, establish root channel patency and glide path with Neoniti GPS no. 15/.03, and complete the channel shaping with Neoniti no. 20/.06 and no. 25/.06. |
Dr. Edit MAROS General Practitioner with a particular interest in Endodontics 3 Rue des Genets
FR-53410 - SAINT-PIERRE-LA-COUR
FRANCE  Clinical case commented by Pr. Jean-Marie Vulcain Case introduction: Tooth #46 was recently restored with a Zirconia onlay. The pre-treatment radiograph highlights the radiopaque cement layer and suggests that the cavity encroaches on the pulp space. There is a corresponding evidence of sclerosis in the pulp chamber. There are also radiographic signs of periapical pathology associated with the distal root. This tooth has been the cause for episodic pain. An Initial Endodontic Treatment is therefore indicated. 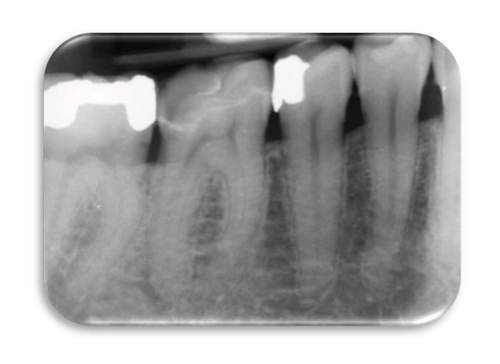 Initial endodontic treatment - Local anesthesia
- Isolation with Rubber Dam
- Accessing pulp chamber through the zirconia restoration
- Detection of the canal orifices and thorough irrigation during and after every stage
- Use of a magnification
- Opening of the root canal orifices with the Neoniti C1 file, and irrigation
- Root channel patency with the Neoniti GPS no. 15/.03
- Establish the Working Length (WL) with an apex locator
- Root canal shaping with Neoniti A1 no. 20/.06, then A1 no. 25/.06, and irrigation
- Drying of the root canals
- Obturation using warm vertical condensation and thermo-compaction
- Final radiographs 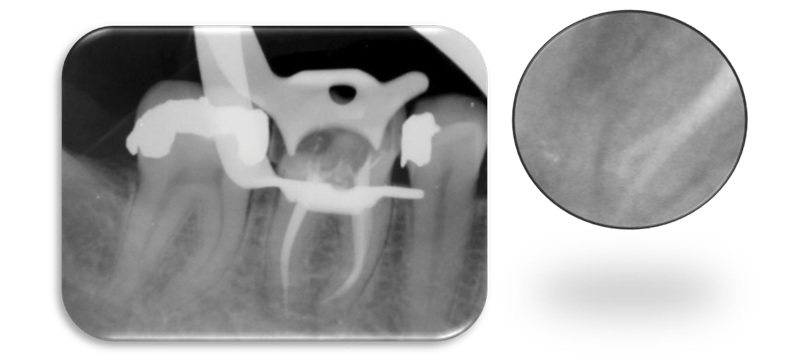 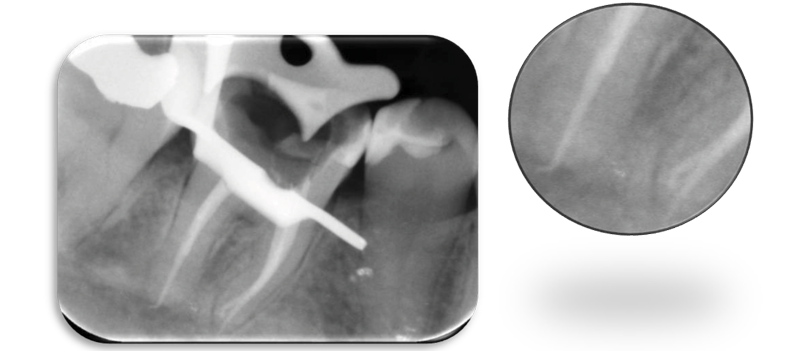 Comments Thanks to its 12% taper and its active length of 10mm, Neoniti C1 no. 25./12 opened 3 root canals while reducing the first curvature and improving the access to the mesial and apical parts of the canals.
Neoniti GPS file eased the path of Neoniti A1 no. 20/.06 and A1 no. 25/.06 and saved time by creating an initial glide path.
Neoniti A1 no. 20/.06 and 25/.06 files finish the root canal shaping in the apical zone while preserving the canal anatomy.
The treatment was successfully completed in a single session. | Dr. Charles-Maximilien THI General Dental Practitioner with an interest in endodontics SCM ALESIA DENTAIRE
10-12 rue de la Tombe Issoire
FR-75014 – PARIS
FRANCE  Clinical case commented by Pr. Jean-Marie Vulcain Case introduction: Lower right second molar #47 has been the source of frequent, acute episodes of pain. A diagnosis of irreversible pulpitis was made. Radiographically there is evidence of caries extending subgingivally in the mesial aspect of the tooth. An Initial Endodontic Treatment is therefore indicated. The per-operative radiograph shows: - Secondary caries below occlusal restoration
- Some root caries mesially – clinically, the tooth is restorable
- The root canals appear to converge apically
- A decrease of the pulp volume
- Complex root canal path with curves and double-curves
- Long tooth roots and hence, long canals
 Initial Endodontic Treatment - Local anesthesia
- Isolation with rubber dam
- Opening of the pulp chamber
- Detection of the canal orifices with the aid of a surgical microscope
- Thorough irrigation throughout the procedure
- Root channel access with Neoniti C1 no. 25/.12 fan then irrigation
- Initial channel scouting using K-files of size #08 – #10 – #15
- Completing glidepath with Neoniti GPS no. 15/.03 and then irrigation
- Measuring the Working Length (WL) using an apex locator
- Preparing the root canals with Neoniti A1 no. 20/.06, then A1 no. 25/.06, and irrigation
- Drying of the root canals
- Calibrated single-cone obturation and direct thermocompaction (McSpadden)
- Post obturation radiograph 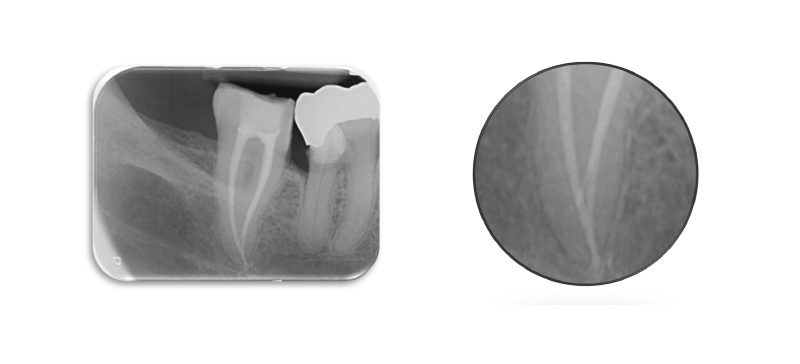 Comments This tooth presents the operator with limited access and thin canals with complex anatomy. The coronal third was accessed using Neoniti C1 no. 25/.12 followed by the creation of a conventional glidepath with K-files #08, #10 and #15. The glidepath was completed using Neoniti GPS no. 15/.03 before completing the shaping with Neoniti A1 no. 20/.06 and no. 25/.06. The postoperative radiograph demonstrates that the natural canal anatomy has been respected allowing complete cleaning, shaping and obturation of the complex canal system | Dr Afzal ALI Endodontist - Associate Professor
Conservative Dentistry and Endodontics Pacific Dental College and Hospital - Airport Rd
UDAIPUR - Rajasthan
INDIA  Presentation of the case: Tooth #35 was tending to percussion test. The patient gives history of attempted endodontic treatment. Endodontic Treatment - Local anesthesia
- Isolation with rubber dam.
-Removal of the temporary restoration.
- Magnification using loupes.
-Access cavity refining.
- Preparation with ultrasonics to identify and expose the canal orifices.
- Patency of channels with a size #10 K file, then with Neoniti GPS no. 15/.03.
- Measurement of the Working Length (WL) & its radiographic verification.
- Shaping of the root canals using Neoniti A1 no. 20/.06;
- Thorough intermittent irrigation.
- Drying of the canals.
- Obturation by warm vertical condensation.
- Finally, placement of definitive restorative material over access cavity of the tooth.
- The treatment was successfully completed in two sessions. 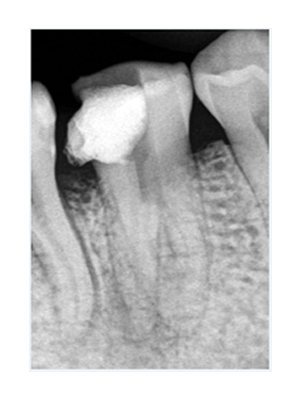 Pre-op radiograph suggestive of attempted endodontic management 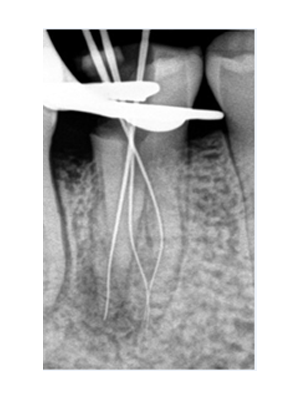 Radiographic verification of WL 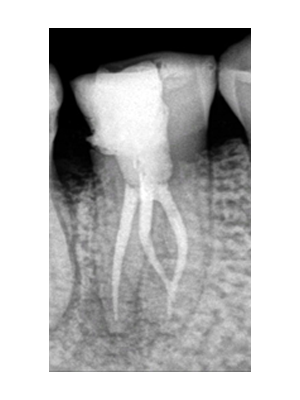 post-op radiograph Comments: - The mandibular premolar is an enigma to the endodontists.
- The incidence of three canals in mandibular second premolar has been reported to be 0.5%. In these cases, the three canal orifices are mesiobuccal, distobuccal and lingual.
- Very careful examination of the pulpal space, preferably with magnification, is recommended to locate any unusual canal orifices.
- Neoniti GPS file eased the path to root apex and saved time by creating an initial glide path.
- Neoniti A1 no. 20/.06 aids in efficient shaping of the root canals along with preserving the original root canal anatomy. |